
 Introduction
Introduction
This article began as a supervision briefing paper and is intended to provide a summary of issues that might be encountered when working with gender, sexuality and relationship diversity (GSRD), a term that includes people who identify as gay, lesbian, bisexual, transgender, queer/questioning, and intersex (LGBTQI) among other possible identities. It is written from a UK standpoint and should be seen in the context of evolving guidelines such as those provided by British Psychological Society (BPS, 2019: see Appendix 1 for a summary). It should be noted, however, that most of the literature referred to has been researched and published in the Unites States (US), so is likely to have some culturally specific limitations. Having said that, the American Psychological Association (2011) guidelines are broadly similar to those of the BPS.
It is hoped that this article will increase confidence in working with GSRD as part of culturally sensitive and competent practice. Terminology in referring to aspects of GSRD varies between authors and over time and continues to change. Where works are cited that refer to specific populations (e.g. LGB individuals) then this briefing has only used the expanded term LGBTQI when the findings are believed to be applicable to more diverse populations. Where terms are used to refer to specific populations, it has tended to stick to the language and terminology used in the original work. The briefing is broken into four parts: an introduction to the concept of minority stress as an explanatory model for differential health outcomes for LGBTQI people; issues relating to non-heterosexual sexual orientation; issues relating to gender identity and transgender issues, including to individuals who identify as intersex; and adaptations to CBT when working with a LGBTQI population.
Minority stress
Evidence suggests that the LGBTQI population overall bears a disproportionate burden of mental health issues relative to the general population (Meyer, 2003). Emerging evidence suggests that mental health problems are higher still among transgender individuals. For example, one survey in the US found that 41% of transgender respondents had attempted suicide at some point in their life (Su et al., 2016). Martell et al. (2003) point out that LGBTQI individuals continue to face high levels of discrimination, prejudice and violence that amount to victimisation and that this experience is linked to an elevated risk for stress-related physical illness, anxiety, depression and suicidality. Dentato (2012) makes a similar point in stating that sexual minority health disparities can be explained in large part by stressors induced by a hostile, homophobic culture, which often results in a lifetime of harassment, maltreatment, discrimination and victimisation that may ultimately impact access to care. Homophobia and heterocentrism can therefore be considered forms of stigma, prejudice and discrimination that contribute to poorer health outcomes in minority groups, including mental health outcomes (Meyer & Frost, 2013).
Pachankis & Goldfried (2004) define homophobia as “an extreme, negative reaction on the part of both heterosexual and homosexual persons to homosexual individuals and homosexual behavior” (p.228) and heterocentrism as “the systemic attitudes and assumptions that operate in a society that understands itself, by default, as purely heterosexual” (ibid, p. 228). Internalised homophobia, or homonegativity, is the felt sense of shame and the urge to hide or disavow a sexual minority identity or same-sex partner preference. Even in people who are accepting of, or proud of, their sexual identity, the experience of having one’s sexual minority status disclosed can lead to feelings of embarrassment, confusion, or shame that might cause the person to disavow their identity or feel a necessity to defend it. Disclosure could be inadvertent, when, for example, being seen by a colleague with one’s partner, or deliberate and against one’s wishes, such as when a person is “outed” (Palma & Stanley, 2002).
Minority stress is the name given to a theory that attempts to describe the relationship between higher rate of stress and poorer health outcomes in disadvantaged communities. Having a minority status, for example as a result of one’s ethnicity or sexual orientation, potentially exposes people to three types of stress: 1) general stresses (e.g. poverty, poor housing etc.), 2) acute, major, prejudice-related minority stresses (e.g. an assault as part of a hate crime or severe acts of discrimination) and 3) chronic, minor, minority stresses (e.g. daily hassles or microaggressions). This combination has been said to contribute to three types of negative outcomes for people from minority sexual communities: 1) a risk of internalised homophobia, 2) increased vigilance for rejection and victimisation, and 3) defensive attempts to conceal one’s minority status. These consequences are themselves stressful and further exacerbate stress. People from communities affected by minority stress are therefore more vulnerable to poorer health outcomes both as a direct physiological consequence of the stress (e.g. the impact of stress on the functioning of the immune system) and as a result of higher-risk health behaviours associated with minority status, such as increased levels of problematic substance use (Figure 1).

Figure 1: minority stress processes
The relationship between risk factors and outcomes is a complex one where negative outcomes, such as increased substance misuse, themselves become increased risk factors. For example, in a study of the impact of minority stress on the mental health and substance use of lesbian and bisexual women in the US, Lehavot and Simoni (2011) described a complex interplay of factors whereby personal gender expression (i.e. whether one presents to the world as butch or femme in appearance and gender role) led to different experiences of minority stress processes such as vigilance, internalised homophobia, and concealment. It was suggested that butch sexual minority women were exposed to more victimisation due to their gender nonconformity, whereas femme women experienced more internalised homophobia, perhaps through efforts to maintain concealment. Negative outcomes reinforced each other, for example problematic substance use increased the likelihood of mental health problems and vice versa. These outcomes were mitigated, or buffered, by the levels of perceived social support and personal spirituality, which contributed to resilience.
Hamilton and Mahalik (2009) found a complex relationship in gay men in the US between experiences of minority stress, masculine gender roles, social norms, and health risk behaviours. The authors reported that in general men engage in more health risk behaviours than women, and gay men engage in health risk behaviours to an even greater extent than heterosexual men. Health risk behaviours included smoking, alcohol use, illicit drug use and riskier sexual health practices, leading, for example, to a disproportionately higher rate of sexually transmitted infections in gay men than heterosexual men. The authors concluded that there were two direct effects: 1) men who adopt traditional, emotionally-restricted constructions of masculinity were more likely to engage in riskier health practices; and 2) gay male social norms regarding substance abuse and riskier sexual practices normalised health risk behaviours. The latter was found to have an even greater influence on health risk behaviours than having a traditional masculine identity. Minority stress was found to have an indirect effect in that minority stress processes (internalised homophobia, vigilance, and concealment) influenced the strength of social norms. For example, gay men who experienced high levels of minority stress were thought to manage their distress through counter-productive emotion regulation practices that involved substance abuse, isolation, and riskier sexual practices.
It was suggested that gay men who had experienced a high level of minority stress may also form a stronger minority in-group identification to buffer the impact of a world they find hostile and rejecting, which makes them more influenced by the behaviour and norms of their peers. In so far as this is also associated with attachment to a highly masculine self-construction, it is possible this creates cohorts of highly in-group identified gay men whose higher risk health behaviours themselves become sources of stress, for example through substance abuse problems and associated mental health difficulties for which they are reluctant to seek help or to change. This model somewhat resembles Hammen’s (2006) stress generation model for depression in which decisions made when not depressed create the circumstances for future stress that may contribute to the stress levels required to trigger further episodes of depression. Recurrent poor mental health outcomes are seen as an interaction between the person and their environment, in which the person’s understandable but unhelpful coping strategies shape the environment to become even more stressful than they originally found it. For CBT therapists who are seeking to help gay men it is important to untangle these various influences in order to develop an idiosyncratic formulation that links the experience of minority stresses, internalised homonegativity and shame, masculine socialisation and a broader personal identity, emotional distress and the function of behaviour to manage distress, and positive coping and resilience, along with the role of their own and their peers’ attitudes to health risk behaviours.
it has been noted that, despite minority stresses, as a whole, the LGBTQI population is quite resilient (Bradstreet et al., 2014). Smith and Gray (2009) noted, for example, that LGBTI individuals are often highly creative in the ways they respond to hardship and tragedy. However, a focus on self-sufficiency can sometimes mean that seeking help from supportive communities is underdeveloped and can lead to a degree of isolation that is itself stressful. Describing LGB individuals, Pachankis and Goldfried (2004) stated that psychological adjustment is probably mediated by the extent to which an LGB individual is committed to his or her sexual orientation identity; the level of his or her contact with other LGB individuals; the amount of family support that he or she receives; and the extent to which an LGB individual is open about his or her sexual identity (Pachankis & Goldfried, 2004). While confining itself to discussions of LGB individuals, these definitions can be read as applying to all areas of gender, sexuality and relationship diversity.
Interventions to lessen the impact of minority stress can take place at both an individual and community-level and are intended to help develop resilience and hardiness in people and the institutions of which they are a part (Meyer, 2003). Despite evidence that mental health institutions and professionals have historically been associated with heterocentric and homophobic prejudices and practices, Pachankis and Goldfried (2004) point out that LGB clients utilise therapy at higher rates than the general population, a finding that extends to transgender clients (Austin & Craig, 2015). Culturally sensitive psychological therapy can help mitigate minority stress for individuals through affirmative practice that focuses on defining adaptive coping strategies, affirming a positive self-identity, and increasing the ability to assess the effect of homophobia and stigma on psychological functioning and health risk behaviour. A positive minority identity increases opportunities for social support and affiliation with others. It encourages and affirms the use of positive coping behaviour and may help clients directly to manage minority stressors. It can help people to dismiss or address perceived or actual homophobia while invalidating unhelpful stereotypes and supporting a positive self-evaluation. In addition, affirmative therapeutic practice might include encouraging clients to establish a support system of other LGBTQI individuals; helping clients become aware of how oppression has affected them; desensitizing the shame and guilt surrounding thoughts, behaviours, and feelings related to one’s identity; and “allowing clients’ expression of anger in response to being oppressed” (Pachankis & Goldfried, 2004, p. 231).
Helpful sociocultural and community interventions might include: changes in the law to address structural inequalities in order to increase feelings of social inclusion and parity with heterosexual couples, for example in legislating for same-sex marriage (as is now the case across the whole of the UK); increased education about minority stress; sensitive and accessible health services, including mental health services; improved recognition and policing of prejudice and discrimination in all its forms; and the provision of safe community centres that can provide culturally relevant information (Meyer & Frost, 2013).
Specific considerations for LGB clients
In order to be well informed and therapeutically helpful, Pachankis & Goldfried (2004) identify a number of specific areas that therapists need to be aware of when working with LGB clients, including: models of identify formation, intimate relationships and parenting, family issues, the unique experiences of under-represented sexual minority populations (such as ethnic minority, religious, older and bisexual populations), and legal and workplace issues.
Defining sexual orientation and identity
Worthington et al. (2002) state that one of the most often cited recommendations for therapists working with LGB clients is to learn a model of lesbian and gay identity development. However, describing the processes behind sexual identity development is made more complicated by the different ways that authors use similar terms and by the differing philosophical underpinnings from which various authors argue their case. For example, a distinction can be drawn between essentialist theories that describe gender and sexual orientation as biologically determined, and therefore fixed or immutable, as opposed to social constructionist perspectives that assert that sociocultural factors inform one’s self-identification. Social constructionist perspectives suggest that sexual orientation and gender identity emerge from interactions with others within a culture (Edwards & Brooks, 1990). Palma and Stanley (2002) state that a social constructionist view can help account for “marked differences in experience, behavior, and personal characteristics within and between sexual identity categories” (p. 75) but have the unintended consequence of seeming to lend weight to the idea that, if gender and sexual orientation are socially formed, then they can also be altered at will to conform to a more socially desirable form.
Dillon et al. (2011) argue that an integration of essentialism and social constructionism may reflect the multi-dimensionality and dynamics of sexual orientation and identity better than either approach alone. For example, the American Psychological Association Task Force on Appropriate Therapeutic Responses to Sexual Orientation (2009), argues that sexual orientation is an immutable physiological predisposition towards patterns of sexual and romantic thoughts, affiliations, affection or desires that are directed towards one’s own sex, the other sex, both sexes or neither sex. Attractions are seen from an essentialist position as being tied to physiological drives and biological systems that are beyond conscious choice. However, these desires are influenced by and given meaning by socio-cultural forces, which is a social constructionist position.
Authors seem to agree that sexual identity and sexual orientation are complex, multifaceted constructs. For Dillon et al. (2011) sexual identity refers to sexual attraction, fantasy, and behaviour, as well as romantic, emotional and social preferences. Sexual orientation refers to patterns of sexual, romantic and affectional arousal and desire linked to physiological drives that are beyond conscious choice, as described above. Sexual orientation identity is self-labelling based on an internalisation of sexual orientation, in other words how one’s desires are understood and their implication for community affiliation, social support, role models and friendships. In Dillon et al.’s model the development of sexual identity is both an individual and social process by which a person recognises, acknowledges and defines their sexual needs, values, sexual orientation, preferences for sexual activities, modes of sexual expression and characteristics of desirable sexual partners. It also consists of an either explicit or implicit understanding of one’s membership of specific social groups, whether those are socially dominant or marginalised, along with the values, norms and beliefs of that group, whether that group is gay, lesbian, bisexual or heterosexual. Within these broad groupings there is potential for identity to be further subdivided. For example, a preference for BDSM sexual behaviours (bondage and discipline, domination and submission, and sadism and masochism) may lead to an identity that is formed at least in part around membership of a community that defines itself through those sexual behaviour preferences.
Rosario and Scrimshaw (2014) describe sexual orientation as a multifaceted concept that includes sexual identity, sexual, romantic and emotional attractions (or desires), and sexual behaviour. Sexual identity refers to the way one self-labels, for example as gay, lesbian, bisexual, queer, questioning, straight etc. They describe identity as “a complex function of how one perceives, situates, and evaluates one’s internal and external experiences in the time, culture, and settings in which one finds oneself” (ibid, p. 557).
Sexual attraction refers to the gender to whom one is attracted, although this comprises both sexual and emotional attraction, so means more than simply the biological similarities or differences of the type of person or people one might wish to have sex with (Rosario & Scrimshaw, 2014). It is sometimes separated from romantic attraction, which is the desire or ability to form an intimate relationship. The ability to form and maintain a stable, mutually satisfying sexual and romantic relationship has been described as “the ultimate indication of commitment to and integration of one’s sexual orientation” (ibid, p. 558) and might have particular significance for gay, lesbian and bisexual individuals in same-sex relationships, given the potential antipathy and obstacles those couples might have to overcome (ibid.)
Meyer (2010) describes four main categories of sexual attractions that consist of: 1) asexual – not attracted to any sex; 2) bi-omni-pansexuals who are attracted to both or all sexes; 3) heterosexuals, who are attracted to the opposite sex; and 4) gay/lesbian, who are attracted to the same sex. These categories appear to be derived from Storms (1980) who conceptualised attractions as aspects of a two-dimensional model (Figure 2). This represented a break from the unidimensional model originally proposed by Kinsey (1948) where sexual attraction is on a 7-point unipolar continuum from exclusively heterosexual to exclusively homosexual. As Storms points out, Kinsey’s model conflates people who have both same-sex and other-sex attraction (i.e. bisexual orientation) and attraction to neither sex (i.e. asexual orientation), although asexuality was represented in the Kinsey scale by a rating of “X”, which indicated “no socio-sexual contacts or relations” (Kinsey Institute, 2019).
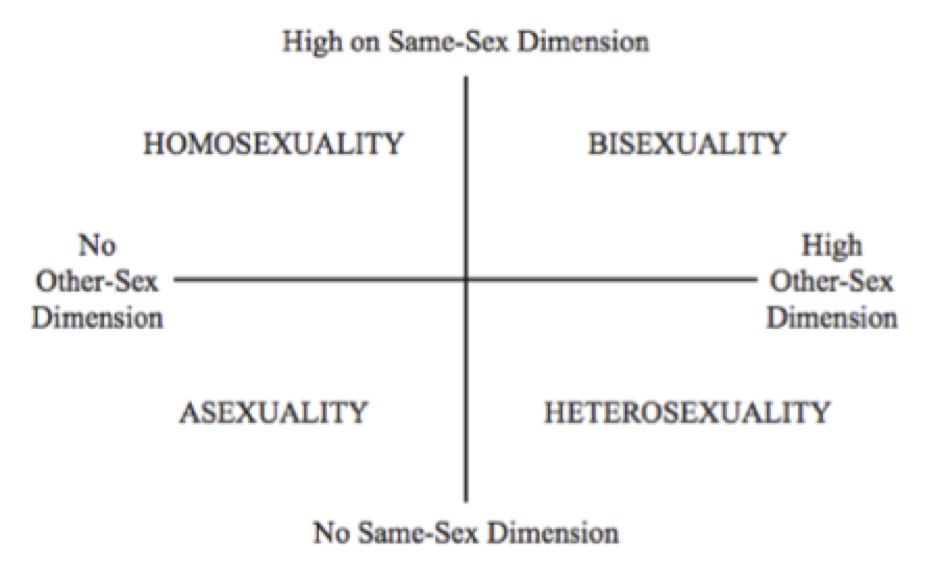
Figure 2: the two-dimensional model of sexual orientation (Storms, 1980).
Storms categorised attractions in a similar way to Kinsey in terms of “acquired erotic responsiveness” where sexual attraction was determined by the content of erotic fantasies: people who are high in both same-sex and other-sex attractions are conceptualised as bisexual, those who are high on same-sex but low on other-sex attractions are homosexual, those high on other-sex but low on same-sex attractions are heterosexual, and those who are low on attractions to both same-sex and other-sex are asexual. Individuals who define as asexual typically experience low levels of desire or attraction but have been shown to display sexual arousal and may enact sexual behaviours, demonstrating the complexity of the relationship between identity, attractions, and behaviour.
Rosario and Scrimshaw (2014) note that a categorical approach, such as Storms’ model, reduces sensitivity to within-groups distinctions, which may be one reason many people may be dissatisfied with identifying themselves within a simple categorical definition that fails to capture the complexity of one’s sociosexual attractions and gender identity. The authors draw attention to the vectors or dimensions of experience, rather than the quadrants. In other words, any individual may be high or low on each of the two vectors of attraction and thus be situated at any point within the two-dimensional space, not just located in a quadrant. However, without categorisation, it is difficult to understand or model commonalities of experience and certainly difficult to organise at a community or political level around the needs and status of marginalised groups without some broader form of identification.
Sexual behaviour means sexual involvement, usually with the object of one’s attractions. Meyer (2010) points out that there is a wide array of sexual behaviours and that there is as much diversity of sexual behaviour within groups as between them. People engage in sexual behaviours for a variety of reasons, and because behaviour is chosen, it can be influenced by many factors. These factors might include what people find emotionally and physically arousing, their moral code and values, their self-esteem, their expectations of self and others in a relationship, the availability of sexual partners, or their personal developmental period (e.g. a willingness to experiment during adolescence). Meyer points out that people who have same-sex attractions may engage in sex in the context of heterosexual relationships to avoid stigmatisation or isolation from friends, whereas people with other-sex attractions may engage in same-sex behaviour opportunistically, as when they are in exclusively same-sex environments. When sexual attractions and behaviour remain consistently in conflict, it is hard to develop a cohesive identity and sense of self.
The data around the ways that identity, attraction and behaviour line up together in an individual (what is termed their concordance) is too detailed and complicated to be explored in detail here, but in general the rate of concordance is rather low. In one study, of a sample of women who reported any adult same-sex sexuality (which was 8.6% of the sample), only 15% reported concordance between attraction, behaviour and identity. For men who reported any same sex adult behaviour (10.1%) the figure was higher at 24% (Laumann et al. 1994, cited in Rosario & Scrimshaw, 2014). It is not entirely clear what this difference in concordance rates signifies, but perhaps that men who have sex with other men are more likely to define themselves as gay and to act on that preference than women, whose sexual identity, behaviour and attractions may be more fluid (Diamond, 2006).
For therapists, it suggests that when discussing sexual orientation in all its facets, it is necessary to maintain a sensitivity to the idiosyncratic meaning a client gives to terms that might otherwise seem straightforward. In short, attraction and desire are universal, timeless, emotional, romantic and sexual; behaviour is diverse and contextual; and identity is the product of the way a person defines themselves in relation to the laws, culture and norms of a particular time and place. A person’s specific socio-cultural context in turn influences what behaviour is permitted and with what consequences, and thus which desires are legitimated, and which are condemned. The ways that people behave, their attractions, and their self-identification may change over time, especially with regard to identity which tends to become more definite, although this phenomenon is perhaps simply the result of more general processes of identity formation than specific to sexual orientation (Rosario & Scrimshaw, 2014).
From a CBT perspective, sexual orientation might best be seen from a pragmatic, heuristic perspective as comprising facets of human experience that can be viewed from separate but interacting perspectives: sexual arousal through a physiological lens; behaviour through a functional approach/avoid (motivational-action) lens, desire through a cognitive (perception and appraisal) lens, and identity through an interpersonal and sociocultural lens. By seeing people’s sexual orientation in a multifaceted way, we can more easily make sense of the fact that people’s arousal may be independent of their experience of desire; that people have sex for reasons that are not necessarily to do with attraction; and that people identify with social constructs that help them achieve and maintain identity coherence and to function interpersonally in a complex social world.
Models of sexual identity formation
Setting to one side the complexity of determining quite what is meant by sexual orientation or identity, there are a number of differing theories of sexual identity formation. Biological theories focus on the development of same-sex and other-sex attractions more than identity. Rosario and Scrimshaw (2014) summarise a number of proposed mechanisms. One set of theories focuses on the possible evolutionary survival function of same-sex attractions in terms of promoting affiliation, sexual pleasure and the inheritance of pro-social traits, however, all evolutionary theorising is highly speculative. Genetic studies have attempted to identify heritable genetic components of sexual orientation but have struggled to produce reliable replicable results. Hormonal effects have also been considered at different points in development: in utero during either the development of sex organs or the development of the brain under the influence of testosterone, and postnatally during puberty and sexual maturation. Unsurprisingly, given the complexity of the construct in question, results have been mixed although there is some evidence for “butch” lesbians having been exposed to elevated testosterone in the pre-natal environment. Similarly, evidence for the fraternal birth order phenomenon and the maternal immune hypothesis, which seems to demonstrate that probability of being a gay man is related to the number of older heterosexual brothers one has, is mixed. In sum, it has been argued that, although there is a strong biological foundation for sexual attractions and a genetic component exists for both men and women, research on potential biological mechanisms underlying homosexuality and bisexuality is “in its infancy” (Rosario and Scrimshaw, 2014, p. 579) and its findings are controversial (Edwards & Brooks, 1999). Taking both social and biological theories into account, Rosario and Scrimshaw suggest it may be best to conclude that there may be multiple forms of same-sex sexual attraction and multiple pathways to sexual orientation.
Stage models of development focus on the process of acquiring an LGB identity rather than same-sex attractions and behaviour per se. They tend to focus on ways of resolving internal conflicts with regard to a gay or lesbian sexual identity, and maintaining that identity as a positive aspect of self across the lifespan (Pachankis & Goldfried, 2004). These models were typically developed in the 1970s and tended to draw on Erikson’s theory of the psychosocial tasks of identity development that suggest that the goal of development is an integrated identity, a perspective that has not always been accepted as a necessary endpoint (Kenneady & Oswalt, 2014).
Stage models are often considered models of the process of coming out. However, the concept of coming out, once seen as a defining part of the experience of developing a minority sexual orientation, is now seen as increasingly limiting and problematic. Disclosing one’s sexual orientation or gender identity is no longer seen as a one-off process that constitutes a final rite of passage but one that involves repeatedly choosing what one chooses to disclose in each new social or familial situation. For young people in particular who have grown up in supportive environments, coming out can be seen as largely irrelevant because they have never felt under pressure to conceal those aspects of identity (Bradstreet et al., 2014). None the less, we should be careful not to conflate the experience of predominantly young, white Western people with those of people from communities that may be markedly more hostile and where “coming out” might still represent a courageous and dangerous declaration of one’s right to individuality and equality. As an example, as of December 2020, 67 UN member states had provision criminalising consensual same-sex conduct including six where the death penalty is the legally prescribed punishment (Brunei, Iran, Mauritania, Nigeria (12 Northern states only), Saudi Arabia and Yemen) and five where the death penalty may be imposed (Afghanistan, Pakistan, Qatar, Somalia (including Somaliland) and the United Arab Emirates) (ILGA World, 2020).
Common characteristics of stage models have been said to include:
- A sensitisation, or pre-coming out, stage: marked by acknowledging feeling different from same-sex peers, especially in terms of nonconformity to socially stipulated gender roles.
- A stage of awareness of feeling sexually different with accompanying defensive psychological strategies: these defensive strategies are used to block recognition of disavowed personal feelings of same-sex attraction. Because maintaining psychological defences is an emotionally demanding and stressful task, it may lead to negative consequences for emotional wellbeing.
- A stage of toleration: this stage may be marked by a less problematic, sometimes tentative acceptance of same-sex attraction, although individuals often lead a “dual life” in that the same-sex attraction is concealed from some people and in some settings. This is also often a stage of emotional and behavioural experimentation accompanied by a growing sense of normality.
- Integration: this stage is one that leads to a positive sense of the self as a lesbian, gay or bisexual person (Ritter & Terndrup, 2002, cited in Pachankis & Goldfried, 2004).
Perhaps the most notable of the stage models is that of Cass (1979, 1984, 1996), whose research is unusual in that it originated in Australia, rather than the US, and also considered the experiences of lesbians as well as gay men. Cass called her model the Homosexual Identity Formation Model and it went through a number of iterations before settling on the following stages:
- Pre-stage 1: an assumption of heterosexuality based on recognition of its normative status
- Stage 1: identity confusion: awareness of a disconnect between previous assumptions of heterosexuality and one’s same-sex attraction or behaviour
- Stage 2: identity comparison: ambivalence and vacillation between acceptance of a potential gay or lesbian identity and denial of this possibility
- Stage 3: identity tolerance: acknowledgement of one’s gay or lesbian sexual orientation with this being viewed either as desirable, undesirable or partly positive. This stage includes increased contact with other people who identify as either gay or lesbian.
- Stage 4: identity acceptance: there are increased interactions with others who share this identity and increased clarity and acceptance of one’s sexual orientation.
- Stage 5: identity pride: a sense of belonging and pride emerges along with an increasing interest in gay and lesbian culture and literature, disclosure of one’s identity, and anger about social stigma and personal discrimination.
- Stage 6: identity synthesis: personal and public sexual identities are synthesised and, while sexual orientation is a source of pride, it is not the sole identity of the person. Self-disclosure becomes automatic, and anger, alienation and frustration become more controlled.
Cass’s model, along with the overall concept of stages in development of one’s sexual identity, has been criticised for its potential limitations. As a linear stage model, it could be seen as being overly simplistic in that it reduces a complex, individual process to a single path of identity formation that fails to consider fluidity in sexual identity. For example, more recent research on adolescent sexual identity formation demonstrates that the coming out process increasingly occurs at an earlier stage and is diverse, including individuals who may have same-sex sexual experiences but not identify as LGB, and those who have no sexual experiences but do identify as LGB (Pachankis & Goldfried, 2004). Stage models have also been criticised on the basis that variability in individual experiences of identity formation is so great that assumptions about what is “normal” or “typical” are effectively meaningless and should be rejected (Savin-Williams & Cohen, 2007).
Stage models that focus on LGB communities may not fully address the ways that sexual orientation definitions are developing, or the experience of heterosexual identity formation, or be empirically substantiated (Morgan, 2013). A further criticism is the lack of inclusion of a diverse cultural perspective. Research on the intersectional identities relating to ethnicity, spirituality/faith and other aspects of social identity, suggest that Eurocentric notions of coming out do not take account fully of the diversity of social and cultural experiences of people from diverse communities, even within the United States, where most research has been done.
Palma and Stanley (2002) therefore suggest that when working with issues of identity formation, therapists should emphasise that there is no uniform path to identity formation but instead focus on the individual nature of the process and the reciprocal interactions between personal and cultural factors that lead to sexual and affectional same-sex attraction. None the less, stage models can still provide useful structures to understand identity formation challenges. When working with clients who are displaying some of the hallmark thoughts, feelings and behaviours of the earlier stages of the coming out process, it can be helpful to validate emerging feelings to encourage self-acceptance. At a practical level, it can help a client weigh up the costs and benefits of disclosing their identity to people or in situations where reactions may be negative or rejecting, especially if the person is in a dependent relationship, for example, when they may suffer the risk of financial hardship, homelessness, or violence if they disclose their sexual orientation or gender identity (Panchaskis & Goldfried, 2004).
Life span approaches offer an alternative model in that they focus on non-heterosexual development as a fluid and complex process influenced by other psychosocial identities. D’Augelli’s (1994) model has six “identity processes” that operate independently and do not occur in stages:
- Exiting heterosexuality
- Developing a personal LGB identity
- Developing an LGB social identity
- Becoming an LGB offspring
- Developing an LGB intimacy status
- Entering an LGB community
D’Augelli (1994) takes a social constructionist perspective where identity is described as a socially mediated subjectivity. This model sees LGB people as having to live lives that comprise multiple psychological identities in order to navigate the demands of a heterocentric culture while simultaneously creating a new identity “oriented around homosocial and homosexual dimensions” (p. 313). The task of exiting heterosexuality therefore, is one in which LGB people create a sexual identity by resistance to the “heterosexist imperative” that sees any deviation from the norm as deviant. D’Augelli describes three sets of linked factors: personal subjectivities and actions, such as personal meanings and behaviour patterns; interactive intimacies with parents, family, peers and partners; and sociohistorical connections consisting of social customs, policy, law and cultural concepts. The model implies that the development of sexual orientation is a lifelong process where the human capacity for developmental plasticity means sexual identity may be very fluid at some points in life and more crystallised at others.
D’Augelli (1994) makes the point that once one has identified and labelled one’s social and sexual attractions the meaning of that label and its implications may be uncertain. Coming out is not an event but a process that starts with the disclosure to the first person one tells and continues throughout life as one continues to assert non-heterosexuality. Developing a personal LGB identity is something that is done interpersonally in social situations where contact with others can help LGB people to learn what their identity means. This is also a lifelong process where being reliably treated as belonging to a community, ideally as part of an affirming support network, helps develop a social identity. Becoming an LGB offspring is the process of adaptation and accommodation that individuals and families must make to adjust to the idea of a nonconforming personal identity, while developing an intimacy status refers to the identification of relationship models and preferences, which might or might not conform to heterocentric stereotypes. Finally, entering an LGB community means to engage with the social and political barriers to development through awareness of the structure of heterosexism and to resist the ways in which its legal and social strictures may continue to be oppressive.
Models of identity formation have tended to assume that the experiences of gay men, lesbians and bisexuals are equivalent. However, research on women suggests that they come out and have same-sex experiences somewhat later than men and that their sexual identity may be more fluid than that of men, suggesting that coming out is a less linear process (Diamond, 1998). Bisexual identity formation is complicated by the fact that it involves the rejection of two recognised categories of sexual identity. There is evidence that people who identify as bisexual face specific challenges, including the lack of a specific community with which to identify and, on occasion suspicion and discrimination within the lesbian and gay communities where it is not uncommon for bisexuality to be regarded as a stage towards full acceptance of one’s lesbian or gay identity rather than a sexual orientation in its own right (Edwards & Brooks, 1999). Dillon et al. (2011) summarise the research findings on bisexual identity development as follows: “(a) bisexuality is a unique and legitimate identity; (b) substantial external pressures to conform to the gay–straight dichotomy may result in considerable confusion, exploration, and uncertainty; and (c) there are important within-group differences among bisexual individuals that have critical influences on sexual identity development” (p. 655).
It should also be noted that heterosexual identity development is an often overlooked and under researched part of understanding gender, sexuality and relationship diversity. In Worthington et al.’s (2002) heterosexual development model, six dimensions of identity formation were described, as follows: 1) perceived sexual needs, 2) preferred sexual activities, 3) preferred characteristics of sexual partners, 4) sexual values, 5) recognition and identification of sexual orientation, and 6) preferred modes of sexual expression. Biopsychosocial influences on sexual identity development include biological processes, such as the age of puberty, the microsocial context of family, friends and peers, gender norms and socialisation processes that encourage conformity, and a dominant culture that includes both negative representation of non-heterosexual orientations and saturation with heterosexual imagery. Heterosexual identity is composed both of individual factors, such as personal preferences, and social identity, in terms of the groups one sees oneself as a member of. In this model, gender and sexual orientation are intertwined in that gender role expression, that is one’s sense of oneself as masculine or feminine, is partly internalised by enacting a heterosexual identity. In other words, the private, individual experience of “real” men and “real” women, i.e. masculine men and feminine women, is expected to consist of attraction to the other sex, while the public, social identity is be seen to be attracted through normative cultural practices that reinforce stereotypical values, beliefs and behaviour, such as getting married and starting a family. The exploration of alternative enactments of sexuality tend to be foreclosed, if not actively restricted and punished, through group affiliation processes that have been described as amounting to “compulsory” heterosexuality.
D’Augelli (1994) makes the point, however, that sexual identity formation for a 20-year old in 1994 would have been a very different process to that of a person in 1974, and of course the same is true of someone now, more than 25 years after that paper was published. This changing social context, and the differences between social contexts both within and between countries, means that identity formation is necessarily a contextual process in which the social, legal and political structures of a society determine what is both possible and normative. When D’Augelli’s model was developed it referred to LGB people, whereas now gender, sexuality and relationship diversity is far more widely defined, expanding the realm of identities that are being considered and the processes across the lifespan that influence their development. For example, the model has also been applied to transgender college students who described similar processes to the ones described by D’Augelli (Renn et al., 2005, cited by Bilodeau & Renn, 2005) and heterosexual identities are not necessarily constrained by traditional models of monogamy, marriage, and children.
Edwards and Brooks (1999) suggest that contemporary models of sexual identity may need to go beyond the concept of identity entirely. They state that the history of sexual identity formation has been at first to pathologise gay and lesbian sexuality and then to try to distinguish it clearly from other forms of sexual expression. They argue that clear distinctions that demarcate certain identities or orientations “may be too confining for the ways in which humans grow into and enact sexuality. The complexity and multiplicity of sexuality may exceed either developmental or sexual identity theory” (p. 53). They suggest that Queer Theory offers a perspective from which to critique identity itself by seeking to “problematize” the binary distinction between heterosexual and homosexual. They offer instead four categories of narrative by which women construct sexual identities: a dominant narrative focused on getting married and having children; a counter narrative as epitomised by identifying as gay or lesbian; a shadow narrative of stories of sexual and physical abuse; and a silent narrative, or experiences of sexuality that are simply not told and thus remain outside of any narrative.
Couple relationships
Panchaskis and Goldfried (2004) report that the literature on LGB couples demonstrates that they function in relationships at least as well as heterosexual couples in that they are as cohesive, flexible, and equal in terms of gender roles, and at least as satisfied as heterosexual couples. Satisfaction and stability are related to similar emotional qualities as heterosexual couples even though LGB couples face challenges that heterosexual couples do not. The authors state that there are a number of stereotypes about same-sex couples that are problematic, including the idea that gay men are emotionally disengaged, sex-driven and non-monogamous, and that lesbian couples tend to “fuse” with one another. While the evidence shows that gay men are more frequently non-monogamous than other individuals, this has been explained by gay men not ascribing an emotional meaning to sex that occurs outside of the primary relationship so that the quality of the primary relationship did not suffer as a result.
Ritter and Terndrup (2000) reported that gender role socialisation affects same-sex couples more than sexual orientation per se. For male couples whose socialisation has discouraged them from developing intimacy skills, problems can be experienced in relationship due to a compartmentalisation of sex and intimacy and an inability to communicate tender and loving feelings. Difficulties in experiencing vulnerability may be exacerbated where there has been a history of rejection, particularly by fathers, or when extreme competition or aggression has been encouraged during development. However, learning to trust and to express intimacy and vulnerability in a relationship can help foster both intrapsychic integrity and interpersonal intimacy, as can a trusting relationship with a therapist where vulnerability can be experienced safely.
Ritter and Terndrup (2000) also stated that female socialisation focuses on defining the self in terms of association with others such that often the needs of others are experienced as one’s own needs and identity is organised around the ability to maintain relationships. They suggested that male models of development, which tend to focus on individuation, separation and autonomy, can lead to women’s focus on relatedness being pathologised as “fusion”. Fusion might therefore be reconceptualised as an adaptive process by which two individuals form a couple. However, if “fusion” persists to the exclusion of a more mature intimacy that balances both couple and individual needs, it can become problematic, especially if one partner starts to desire more independence than the other is able to tolerate. For same-sex couples, as with heterosexual couples, achieving a dynamic balance between connectedness and separateness is an ongoing developmental task that is engaged with repeatedly over the lifespan.
Longitudinal research by the Gottman Institute (2021) reported that relationship satisfaction and quality were about the same across all couple types that were studied (heterosexual, gay, and lesbian) but that the ups and downs of lesbian and gay relationships may occur in a social context where the couple is isolated from family, or where they experience workplace prejudice or other unique minority stresses. Their research suggested that gay and lesbian couples use more affection and humour when bringing up a disagreement and partners receive it more positively. Gay and lesbian couples tended to use fewer controlling or hostile emotional tactics and displayed less belligerence, domineering and fear with each other. In conflict, positive comments have a more positive impact and negative ones have less impact as they are not taken so personally as they tend to be in heterosexual couples. These findings led the researchers to conclude that fairness and power-sharing between partners is an important component of gay and lesbian relationship strength. However, while lesbians were more emotionally expressive than gay men, both positively and negatively, gay men needed to be careful to avoid negativity in conflict as repair strategies could be less effective.
Parenting
In 2005, the American Psychological Association Research stated that there were no studies that had found the children of same-sex parents to be disadvantaged in any significant respect relative to the children of heterosexual parents. Panchaskis and Goldfried (2004) stated that research on parenting by gay and lesbian parents shows that children of same-sex parents do not differ from children of heterosexual parents in terms of gender identity, gender-role behaviour, and sexual orientation and overall are similar in terms of psychological, behavioural, emotional and intellectual functioning to the children of heterosexual parents. However, Marks (2012) stated that there were major flaws in the studies that provided this basis of comparison, especially in that they were small scale and unrepresentative, often with no adequate control group, or where evidence was based on the self-report of participants who may have been biased.
This remains a controversial and politicised debate, especially in the US. At least one author (Fitzgibbons, 2015) has stated that “An objective examination of social science research into how families function reveals clearly that children do best when raised by both a mother and a father” (p. 335), although this point is made not just in relation to gay and lesbian parents but in support of traditional, heterosexual family structures overall. However, even if true that children of same-sex parents have statistically poorer outcomes, for example in terms of likelihood to graduate from high school, as Allen’s (2013) analysis of data from both the US and Canadian census seemed to show, the reasons for this difference have not been identified. It is therefore impossible to know whether this is as a result of, for example a lack of diversity of gender within the home or from experiences of discrimination and prejudice as a result of the stigma of having same-sex parents. Whatever the reality of any possible statistical difference in outcomes, the priority of psychological therapists is to identify the challenges facing clients and to support them in overcoming them, not to prejudge their fitness as parents on the basis of their sexual orientation or gender identity, given that the gender of parents has been shown to have minor significance for the psychological adjustment and social success of children (Biblarz & Stacey, 2010).
Families of origin and families of choice
Most LGB people are raised in heterosexual families. When LGB people come out to their families, it has been suggested that the family itself has to go through a schema shift that is tantamount to coming out as parents of an LGB offspring. This process may be disorientating as the new information causes the family to review its history in the light of the new information. When working with clients who are considering coming out to family, it has been suggested that it is important to bear in mind the family’s values concerning sexual orientation, the effect of those values on the relationship between the disclosing family member and the family member who receives the news, and the conflict resolution mechanisms available to family members (Panchaskis & Goldfried, 2004). Where families of origin may not be able or willing to offer the support that an LGB person needs, families of choice, that is the more extensive support network that the person has created that do support their identity, may constitute meaningful relationships that buffer minority stress. None the less, family support is often a primary source of support in fostering self-esteem and self-respect for one’s identity.
Ageing
The experiences of older LGBTQI individuals has been less well researched but it is likely that they experience specific stresses associated with sexual orientation and gender identity issues and with ageism, not least due to the likelihood of encountering less accepting attitudes in an older cohort of peers who were socialised in a culture that may well have been strongly homophobic. There is some evidence that gay men experience accelerated ageing, where they consider themselves old considerably earlier than other men, perhaps due to an investment in idealised standards of youth and beauty, whereas lesbians tend to view ageing more positively, perhaps due to greater social support and a higher social status among peers of diverse ages (Hash & Rogers, 2013). When older LGBTQI people seek support, for example when they require residential care, there may be challenges finding sensitive care homes or carers and this may expose people to further prejudice, stigmatisation and discrimination that reduces quality of life and acts as a vulnerability factor for poorer health outcomes (Panchaskis & Goldfried, 2004).
As the population of older adults continues to grow in Western European and North American societies, these issues are likely to become increasingly salient. Older LGBTQI adults sometimes describe themselves as “twice hidden”; that is, invisible due to their age and their identity (Hash & Rogers, 2013). However, despite experiences of significant adversity both historically and as they get older, many individuals display considerable resilience, including adaptability, self-reliance, advocacy skills, crisis competence, and gender role flexibility that are assets in navigating the process of ageing. Erikson’s (1950) psychosocial model of development may be relevant to understanding the challenges facing this population. Its final stage consists of “Ego Integrity versus Despair”, where ego integrity is a process whereby reflection on one’s life leads either to acceptance or despair. Acceptance may be a challenging process for those people whose lives have been marked by discrimination, prejudice and, often loss, not least due to the heavy toll on the lives of friends, family, lovers and peers as a result of the AIDS epidemic during the latter decades of the 20th Century. Some LGBTQI people may find themselves reflecting on lives that have felt inauthentic due to the limited choices available to them and may struggle to find acceptance of opportunities that were missed or never available.
Religion
LGBTQI people who have a religious faith may find themselves in conflict with the teachings of their religion that are intolerant of or condemn same-sex attraction, behaviour and relationships. Coping strategies to resolve these conflicts may be more or less successful or appropriate. For example, some LGB people may seek out discredited and unethical so-called gay conversion therapies, whereas others might reinterpret seemingly homophobic religious teachings or join a more tolerant and accepting denomination.
Ethnicity
The issue of ethnicity and how it intersects with gender, sexuality and relationship diversity is an important one and there is only scope to touch on it briefly here. Intersections of sexuality and ethnicity can be a source of great stress not least because it can be the cause of two sources of minority stress. LGBTQI people may also experience the stress of heterocentric intolerance towards their sexual orientation or gender identity within their own ethnic communities and may feel forced to choose between participation in their ethnic community and accepting and living out their sexual orientation. Within some ethnic communities same-sex behaviour may not necessarily be seen as indicative of being gay, lesbian or bisexual, so it is important to identify how clients make meaning from their lived experience, rather than applying labels to behaviour or identity that might not be culturally appropriate. As previously described, associating certain sexual behaviours with sexual identities is problematic in that there is no universal social meaning that can be attached to a specific act with a specific person. Sexual identities are constructed in specific historical and sociocultural contexts that may have limited applicability beyond the context in which they evolved and typically function (Edwards & Brooks, 1999).
Legal and workplace issues
The legal situation facing LGB people and the status of their relationships in the UK and their rights at work continues to evolve. It is recommended that for up-to-date information practitioners consult a reputable source of information. Citizens Advice is a useful resource that provides information on legal rights concerning family law, workplace discrimination, and hate crimes covering all four constituent parts of the United Kingdom.
Transgender issues
Bradstreet et al. (2014) assert that “Despite prevailing cultural understandings that male and female gender identities are fixed and easily assigned…gender identity and expression is best seen as a flexible socially-constructed spectrum rather than as a fixed binary classification” (p. 22). They conclude that gender independent, gender diverse, or gender variant are appropriate ways of describing the experiences and identities of people who define themselves as transgender, rather than the “pathologising” language of “gender dysphoria” or “gender identity disorder”. Martell et al. (2003) state that, while an understanding of terminology is important, there are many debates over it and not all definitions are accepted by those with expertise on a transgender population. In contemporary usage, transgender refers to people whose gender identity conflicts with:
- Biological sex assignment, and/or
- Societal expressions for gender expression as male or female
Transexual refers to people who seek to change their primary social gender roles and their physical bodies. Gender non-conforming or gender variant refer to people whose gender social role does not fall into convectional parameters. Intersexed people are individuals whose genital structures are different from those generally assigned at birth as either male or female. Questioning is a term that includes any individuals who are exploring their gender and/or sexual identity and expression (adapted from Martell et al., 2003).
Bilodeau and Renn (2005) state that in the West transgender identities can include: transsexuals, transvestites, male and female impersonators, drag kings and queens, male-to-female (MTF) persons, female-to-male (FTM) persons, cross-dressers, gender benders, gender variant, gender nonconforming, and ambiguously gendered persons. Where “coming out” is the primary metaphor for a process of disclosing one’s sexual orientation as part of an identity process, “transitioning” is the word most associated with gender identity processes. Transitioning means different things to different individuals but at its core is the movement to live in a way that affirms a chosen gender identity rather than the gender identity assigned at birth. Most transgender people will perform a social transition which could involve expressing their gender identity more openly, disclosing their preferred gender identity to others, and informing people of their preferred name and personal pronouns. Some may seek or engage in medical or surgical procedures to alter their bodies and their physiology to more closely align themselves physically with their preferred gender identity, including through gender affirmation surgery. Gender affirmation processes may therefore include social, legal, medical and/or surgical interventions and changes. Gender affirmation may involve a number of stages or processes, including witnessing, which is having one’s preferred gender identity affirmed by others, and mirroring, which is to see oneself in others who are in some important way like us (Devor, 2004). For non-binary transgender people, gender affirmation surgery may be considered counterproductive as the only choice offered is to be either male or female as a binary choice. The privileging of binary male-female identities has been described as cisgenderism, which “assumes that gender is universally experienced as a permanent and intrapsychic identity, rather than as a shifting relational status, and that each “normal” person has a single “real” gender that does not shift across the lifespan” (Blumer et al., 2013, p.269).
Lev (2004) contrasts two models of sex, gender identity, gender role and sexual orientation. The first is a bipolar model, i.e. one can be only one or the other of each pole), the second is one that sees each of those attributes on a continuum. In the bipolar model one has a sex that is either male or female, a gender identity that is either a man or a woman, a gender role that is either masculine or feminine, and a sexual orientation that is either heterosexual or homosexual. In a traditional model of gender identity and sexual orientation, gender-conforming, masculine, male men are attracted to gender-conforming, feminine, female women, and vice versa. In a dimensional model, sex, gender identity, gender role expression, and sexual orientation are each on a continuum and not mutually exclusive so that moving in one direction does not constrain one from moving in the other direction. A dimensional model allows for much greater flexibility in gender identity, gender role expression, and sexual orientation and would help to make sense of the low concordance rates between attraction, identity and sexual and romantic behaviour.
Lev (2004) goes on to describe a developmental model of transgender emergence that consists of a complex interaction of developmental and interpersonal transactions across a series of stages of adaptation that may not be linear. The first stage consists of a growing awareness of gender variance; the second stage is one of seeking information and reaching out to gain education and support. The third stage is one of disclosure to significant others, and the fourth is an exploration of various transgender identities in order to self-label an appropriate identity. The fifth stage is an exploration of transition options, including possible bodily modification, and finally the sixth stage is the ability to integrate and synthesise a transgender identity after transition.
In the psychiatric literature, DSM-5 uses the term transgender to refer more narrowly to a mismatch between the gender assigned at birth and experienced gender. Gender dysphoria is the distress that can result from that incongruence. Gender identity is regarded as specifically different from gender expression (e.g. masculine and feminine gender expression through clothing choices) and from sexual orientation (American Psychiatric Association, 2020).
The diagnostic criteria for gender dysphoria in DSM-5 (American Psychiatric Association, 2013) are as follows:
- Marked incongruence between one’s experienced/expressed gender and their assigned gender, lasting at least 6 months, as manifested by at least two of the following:
- A marked incongruence between one’s experienced/expressed gender and primary and/or secondary sex characteristics (or in young adolescents, the anticipated secondary sex characteristics)
- A strong desire to be rid of one’s primary and/or secondary sex characteristics because of a marked incongruence with one’s experienced/expressed gender (or in young adolescents, a desire to prevent the development of the anticipated secondary sex characteristics)
- A strong desire for the primary and/or secondary sex characteristics of the other gender
- A strong desire to be of the other gender (or some alternative gender different from one’s assigned gender)
- A strong desire to be treated as the other gender (or some alternative gender different from one’s assigned gender)
- A strong conviction that one has the typical feelings and reactions of the other gender (or some alternative gender different from one’s assigned gender)
- In order to meet criteria for the diagnosis, the condition must also be associated with clinically significant distress or impairment in social, occupational, or other important areas of functioning.
In their chapter on research and controversies in the field of transgender identities, Sanchez and Vilain (2013) identify a number of areas of controversy in the field of transgender identities including: 1) the diagnosis of Gender Identity Disorder (now deprecated in DSM-5), 2) the concept of autogynephila as a way of conceptualising one of two groups of distinguishable male-to-female transsexuals and, 3) gender nonconformity in children. These areas will now briefly be reviewed with implications for UK practitioners.
Gender Identity Disorder
Transgender activists assert that a diagnosis of Gender identity Disorder (as was the case in DSM-IV) constituted medical malpractice as it pathologises transgender identities and manipulates and controls transgender people and their bodies (Cooper, 1999). This diagnosis has been removed from DSM-5, which, as we have seen, now focuses on gender dysphoria. None the less controversy remains about whether medical practitioners should be the gateway to gender affirmation surgery due to the implication that transgender identification is a psychiatric condition that needs to be professionally assessed in order to be validated. In the UK it was proposed that changes to the Gender Recognition Act of 2004 would allow people to self-determine their gender in order to receive the Gender Recognition Certificate (GRC) required to legally change one’s gender. However this proposal was dropped after consultation. In order to obtain a GRC, a person needs to have a medical diagnosis of gender dysphoria from an approved medical practitioner; provide a medical report on any treatment they have had; provide evidence that they have lived in their new gender for at least two years; have the consent of their spouse or civil partner (if they have one); and to make a statutory declaration that they intend to live in the acquired gender until death. The application is then decided on by a judge and medical professional together (UK Government, n.d.).
Autogynephilia
Sanchez and Vilain (2013) note that there are typically two distinct groups of MTF (male to female) transexuals: those who seek to transition in childhood or adolescence, and those that seek to transition in mid-life. The former group, at least in the US, tends to be non-white, more stereotypically feminine, attracted to men, and find it easy to pass as a woman, whereas the latter group tends to be white, more stereotypically masculine, attracted to women, and find it harder to pass as women. It was proposed that the former group’s gender dysphoria is unrelated to sexual orientation whereas the latter group’s experience of transgenderism is predominantly related to sexual arousal. Blanchard (1985, cited in Sanchez & Vilain) described this as a paraphilia and gave it the name autogynephilia, which translates to self-woman-love. As with other paraphilias, this condition is virtually exclusive to males. The theory has been controversial; Serano (2020) criticised it as having been scientifically disproved and being “inconsistent with the basic tenets of feminism” for relying on “essentialist, heteronormative, and male-centric presumptions about women and LGBTQ+ people” (p. 763). However, Lawrence (2017) states that “the descriptive and clinical value of Blanchard’s theory [of autogynephilia] remains undiminished…autogynephilia continues to be useful to researchers and clinicians despite its failure to achieve universal acceptance” (p. 52).
Gender dysphoria in children
Sanchez and Vilain (2013) point out that knowing how to respond to a child who is expressing gender nonconformity is a contentious issue. On the one hand are professionals who argue that children should be allowed to start transitioning earlier and recommend puberty-delaying medication so that secondary sexual characteristics have not developed. On the other hand, are those professionals who believe that the nature of many gender-nonconforming children’s gender identity is likely to resolve in to one that is congruent with their birth-assigned gender. A figure of 80% has been widely cited for those children who will ultimately identify as cisgender and “desist” from their gender nonconformity. One study concluded that only children with extreme gender dysphoria are likely to seek gender affirmation surgery, while children with less persistent and intense gender dysphoria are likely to identify as gay, lesbian or bisexual without gender dysphoria (Wallien & Cohen-Kettenis, 2008). However, both that research, and studies showing similar outcomes, have been criticised on methodological, theoretical, ethical, and interpretive grounds, with the suggestion being made that a more germane question than how children’s gender identify develops over time, is to ask how children can best be supported as their gender identity develops (Temple-Newhook et al., 2018). It could also be argued that these two questions are not mutually exclusive and both might have relevance. In longitudinal research it has been shown that self-identified lesbian or gay adolescents were more likely than heterosexual counterparts to have shown high levels of gender nonconforming behaviour in childhood, which occurred before the age of 5, suggesting that gender nonconformity in behaviour is not necessarily related to gender identity, but prospective for sexual orientation (Kung & Hines, 2017). These different views seem to highlight how complicated and interlinked are the concepts of assigned sex, gender identity, gender-role expression, and sexual orientation. With regard to practical considerations in the UK, as of December 2020 the UK High Court has ruled that children under 16 are unlikely to be able to give informed consent to treatment with puberty-blocking medication leading to a pause in all new referrals for puberty blockers and a review by the NHS into gender identity services for children and young people.
Public controversies
In the public domain there remains intense controversy over the expression of views that have been described by transgender activities as transphobic and thus hate speech that oppresses and marginalises people who identify as transgender. Critics of this point of view, who are sometimes described using the derogatory term TERF (trans-exclusionary radical feminist), assert that attempts to define criticisms of transgender concepts are attempts to limit freedom of speech and academic freedom. At the root of these disputes appears to be a difference regarding how gender and sex are understood. Those who hold an essentialist view of sex as based in a biological reality, differentiate between male and female and thus men and women on this basis. Those that hold a social constructionist view of sex and gender regard both sex and gender as flexible, non-binary, and socially determined. On the one hand authors such as the British academic Kathleen Stock state that transwomen are male and that if transwomen are allowed into female-only spaces this puts women at risk; on the other are those who believe that the publication and dissemination of these views makes academic life so stressful that they are unable to participate in it and thus effectively silenced and excluded (Flaherty, 2019).
Intersexuality
Although unrelated to transgender issues, intersexuality is often included in discussion of it, perhaps because historically genital surgery has been a common medical procedure for people either seeking gender affirmation surgery or where surgery has been performed to “correct” ambiguous genital structures. The concept of intersexuality relates to people where it is not easy or straightforward to assign a sex at birth or where a mixed reproductive system is evident, as can occur as a result of atypical sexual differentiation processes in utero. These may be a consequence of hormonal under- or over-exposure, or due to genetic conditions. Traditionally most infants with intersex conditions have been treated with corrective gender surgery that is intended to align sexual anatomy with presumed gender, although these procedures have been challenged. This model of “corrective” surgery has been described as a concealment-centred approach and has been contrasted with a patient-centred approach in which intersex bodies are seen as a relatively common variation. This has led to the encouragement of a “wait-and-see” approach that delays any surgical interventions until the child develops a stable gender identity (Lev, 2004). In a patient-centred approach, people with intersex conditions are regarded as having the right to self-determination and early intervention that takes place before they are able to consent to them are a violation of those rights. Where surgery has been performed the consequences may be gender dysphoria, embarrassment about their bodies, or feelings of deep shame (Bradstreet et al., 2014).
Psychological therapy and CBT with LGBTQI populations
Safe, effective and professional practice with people who identify as LGBTQI is an example of working in a culturally competent manner with a diverse population. Cultural competence requires practitioners 1) to be knowledgeable about a client’s culture so that formulations take account of cultural norms and expectations without asking clients to perform the potentially stressful task of educating the practitioner about it; and 2) to consider the unique features of the person that are informed by, but independent of, their cultural background. Having said that, Bradstreet et al. (2014) state that the “basic rules of listening to your client and creating a safe affirmative space for them” (p. 4) are the same as would be used with any client.
Pachankis and Goldfried (2004) suggest that therapists address potential therapeutic biases associated with heteronormative assumptions, pointing out that less than appropriate treatment occurs when therapists assume a client’s heterosexuality or, on disclosure of a sexual minority status, attempt to make that the therapeutic issue, even when that is not the issue the client wishes to address. To identify potentially unhelpful attitudes, Martell et al. (2004) suggest that therapists raise their self-awareness by asking themselves the following questions when working with LGB clients (and by extension all LGBTQI clients):
- Do I believe that LGB people are immoral or disordered simply because of their sexual orientation?
- Am I anxious when I meet a client who exhibits gender-atypical behaviour (e.g., a man with strongly feminine characteristics)?
- Do I avoid asking clients about their sexual orientation?
- When clients discuss dating or families, do I assume their partner is of the opposite sex?
- Do I feel uncomfortable discussing sexual acts between two people of the same sex?
- If I am uncomfortable with such discussion, do I make attempts to discourage clients from disclosing details of their sexual behaviour?
- Am I more likely to assume psychopathology if I know my client is LGB?
- Do I diagnose personality disorders more frequently if my client is LGB?
- Do I perceive LGB couples to have more problems than heterosexual couples?
- Do I miss some of my clients’ problem behaviours because I am afraid to discuss their sexual orientation, sex life, or relationship status? (p. 204).
Bradstreet et al. (2014) pose further questions for self-reflection. These make explicit that heterosexuality is a sexual orientation and cisgender a gender identity, rather than focusing on LGBTQI identities as being different from a taken-for-granted norm:
- What views of LGBTI people did you grow up with?
- What were some of the sources of these views?
- When and how did they change?
- How and when did you decide about your own sexuality?
- If you are heterosexual did you make a conscious choice?
- When did you ‘come out’ as a heterosexual, bisexual or homosexual?
- How do you understand the links between biology and sexual orientation and gender identity?
- What do you believe about bisexuality and why?
- What makes you think of yourself as a man or a woman?
- How do you think about the role of gender in your life?
Therapists who identify as heterosexual might like to reflect on the questions posed by Martin Rochlin (1995), who in the 1970s devised “The Heterosexual Questionnaire” as a pedagogical tool to help students explore heterosexual privilege and assumptions, stereotypes and stigma regarding LGBTQI people and communities. Various adaptations have been developed, but in its original form (as far as can be discovered) it reads as follows:
- What do you think caused your heterosexuality?
- When and how did you decide that you were a heterosexual?
- Is it possible that your heterosexuality is just a phase you may grow out of?
- Is it possible that your heterosexuality stems from a neurotic fear of others of the same sex?
- If you have never slept with a person of the same sex, is it possible that all you need is a good gay lover?
- Do your parents know that you are straight? Do your friends and/or roommate(s) know? How did they react?
- Why do you insist on flaunting your heterosexuality? Can’t you just be who you are and keep it quiet?
- Why do heterosexuals place so much emphasis on sex?
- Why do you heterosexuals feel compelled to seduce others into their lifestyle?
- A disproportionate majority of child molesters are heterosexual. Do you consider it safe to expose children to heterosexual teachers?
- Just what do men and women do in bed together? How can they truly know how to please each other, being so anatomically different?
- With all the societal support marriage receives, the divorce rate is spiralling. Why are there so few stable relationships among heterosexuals?
- Statistics show that lesbians have the lowest incidence of sexually transmitted diseases. Is it really safe for a woman to maintain a heterosexual lifestyle and run the risk of disease and pregnancy?
- How can you become a whole person if you limit yourself to compulsive, exclusive heterosexuality?
- Considering the menace of overpopulation how could the human race survive if everyone were heterosexual?
- Could you really trust a heterosexual therapist to be objective? Don’t you feel s/he might be inclined to influence you in the direction of his/her own feelings?
- There seem to be very few happy heterosexuals. Techniques have been developed that might enable you to change if you really want to. Have you considered trying aversion therapy?
- Would you want your child to be heterosexual, knowing the problems that s/he would face?
CBT can be conducted as a culturally sensitive therapy based on a number of factors: it is based on an individualised case conceptualisation; in CBT, the issues addressed are based on the client’s specific context; CBT is collaborative, and the client is regarded as the expert on their life; and, CBT seeks to empower clients and is not “done to” the client but “done with” them as a way of helping a client explore the ways their behaviour contributes to heightened distress (Pantalone et al., 2010).
Balsam et al. (2019) state that, while CBT techniques are similar for people of all sexual orientations and gender identities, there are culturally sensitive adaptations that can be made to enhance treatment effectiveness. The authors note that the history of behaviour therapy includes the development and dissemination of discredited and unethical behaviour modification therapies that sought to change a minority sexual orientation through the use of aversion therapy. This history should be taken into account when working with clients who may be understandably suspicious about the ways that the history of psychotherapy and psychiatry have colluded with heteronormative and homophobic narratives and practices.
When developing a case conceptualisation based on a standard CBT assessment, therapists should routinely ask about sexual orientation and gender identity, just as they do about other aspects of social identity, such as ethnicity. It can be helpful to notice and avoid the temptation to make assumptions about the gender of a person’s partner, if they have one, or their attractions or sexual behaviour. Sexual behaviour and attractions should not be assumed to reflect identity because, as we have seen, a person’s behaviour has its own unique meaning for each individual. When discussing identity, it can be helpful to explore the ways that sexual orientation and gender identity intersect with other identities that are salient to that person. Where there are discrepancies between identity, behaviour and attractions, such as when a person is having same-sex experiences but does not identify as gay or lesbian, or vice versa, it is helpful to explore them with a view to understanding their meaning for the client. Assessment should also include exploration of gender identity (as compared to identity assigned at birth), gender expression (relative to gender expression norms), and gender transition experiences and desires, if any. (Balsam et al., 2019).
When asking about sensitive areas with any client, it can be helpful to preface inquiries with a permission-seeking question and a statement that normalises this area of questioning. For example, therapists might state that they routinely ask about sexual orientation and gender identity and ask directly whether the person would have any objection to being asked about that area of their identity and experience. It can then be helpful to ask open-ended general questions about the person’s current or most recent sexual partner (if any) and how they wish to be referred to in terms of gender. Clients generally appreciate being asked permission, or at least are understanding and tolerant of these questions when they are given a rationale for them, such as letting clients know that we want to understand them on their own terms and not make unhelpful assumptions. Similarly, it can be helpful to ask about the degree of satisfaction with a person’s relationship status and sex life. The acronym PLISSIT (Annon, 1976) describes a structured way of asking about sexual functioning and sexual satisfaction, as follows:
- Permission (P)
- Ask permission to discuss sexual functioning: give a rationale for asking
- Limited information (LI)
- Where there is a problematic deficit in knowledge or a belief in unhelpful myths, give relevant information and normalise
- Specific suggestions (SS)
- Suggest coping strategies or ways to access further information, for example relevant literature, websites etc.
- Intensive therapy (IT)
- Refer to psychosexual or relationship support if beyond the scope of individual expertise or competence
However, as previously noted, therapists should not assume that sexual orientation or gender identity are prominent features in the aetiology or maintenance of the presenting problem or a part of the reason for seeking treatment.
In developing a longitudinal formulation, it can be helpful to enquire sensitively about the “coming out” process using either stage models or tasks of identity formation models to inform understanding of developmental processes, rather than trying to shoehorn the client’s experience into a model. An assessment of current context needs to take account of stresses, such as experiences of discrimination, and supports, such as belonging to a supportive community, and identify how these impact on the presenting problem or on levels of distress and capacity to function.
There is some evidence that LGBTQI people have an increased risk of suicide and that they are at increased risk of violence, so it is important to conduct a sensitive but thorough assessment of risk of harm in all its forms (Bradstreet et al., 2014). If suicidality is disclosed, it is important to assess both the motive for suicide, for example surcease of unbearable psychic pain, and the circumstances that give rise to it, and, if relevant, to understand the stresses and pressures in terms of minority stress processes such as internalised homonegativity. It is also important to understand whether the client is at risk from others and needs support to ensure their safety, for example if they are at risk of violence, bullying, harassment or being made homeless. These external risks may derive from a disclosure, or fear of disclosure, of their LGBTQI status, whether that occurs by choice or inadvertently through being “outed”. Protective factors for young people at risk of suicide include family connectedness, perceived caring from other adults, and school safety (Haas et al., 2010).
In general, gender neutral questionnaires, such as the PHQ9 or GAD7 can be used as with any client group but care should be taken with some questionnaires whose questions may imply a heterosexual or cisgender identity, or that have had their norms developed on populations that are not sufficiently representative.
Affirmative CBT needs both to be explicitly non-judgemental and to recognise that mistakes in therapy, such as inadvertently mis-gendering a client, may be experienced as microaggressions to which people are understandably sensitive. Asking for feedback and engaging in relationship repair strategies may need to be attended to sensitively. When considering treatment interventions, using functional analysis to elicit the costs and benefits of behaviour, such as avoiding disclosing one’s sexual or gender identity, need to be considered in the context of a world in which discrimination and prejudice are parts of lived experience. At the same time, while respecting the client’s experience, it can be helpful to explore through guided discovery the assumptions clients are making about the likelihood of certain outcomes occurring in this context, even if previous experience has taught clients to be wary or vigilant. The sensitive use of discursive Socratic questioning can also be used to explore internalised homophobia or transphobia (Balsam et al., 2019). A focus on strengths and resilience more than deficits, risk and vulnerability, can help to affirm existing capacities and support as a basis for going on to develop increased coping skills and resources (Smith & Gray, 2009).
Austin and Craig (2015) describe a transgender affirmative approach to CBT that takes into account the historical context of transgender issues in mental health care and the minority stress framework of victimisation, discrimination and microaggressions, and current mental health disparities. It also focuses on identifying resilience and the unique experience and perspective of each transgender individual. The authors suggest that when working with transgender clients, practitioners make an explicitly affirmative statement about taking an inclusive approach to gender; use gender neutral language and state their own preferred gender pronoun; and clarify their therapeutic role and purpose, for example as a trans-affirmative advocate seeking to support client self-determination.
Austin and Craig (2015) suggest that an adapted transgender affirmative CBT practice should focus on psychoeducation, modifying problematic thinking styles, enhancing social support, and preventing suicidality. These tasks should be undertaken while creating a “space for clients to safely explore, understand, and inhabit individual experiences of gender” (p. 21). Psychoeducation focuses on helping transgender clients identify and recognise experiences of transphobia and its consequences for them as individuals in terms of stress, anxiety, depression, hopelessness, and suicidality. It is hoped and intended that as a consequence they will come to see themselves as people who are doing their best to cope in stressful and hostile circumstances, rather than disordered or pathological. Following psychoeducation, transgender clients are encouraged to challenge internalised transphobic self-evaluations and beliefs in order to identify the effect of these cognitions on mood and on unhelpful or maladaptive coping behaviour. Hopelessness associated with cognitions such as “I will never fit in this world” can be addressed by strategies such as the creation of a tans-affirmative Hope Box, which is a physical or virtual container in which the client places objects that inspire a sense of hope in a more fulfilling future. Encouraging clients to connect with trans-affirming support groups or organisations can also engender hope, as well as coaching to support the development of interpersonal strategies for maintaining relatedness to others.
In a study of resilience among transgender youth Grossman et al. (2011) identified that higher self-esteem, a higher sense of personal mastery, and greater perceived social support were predictors of positive mental health outcomes, whereas the use of emotion-oriented coping predicted negative mental health outcomes. While acknowledging that the sample on which this study was based was very limited, the results suggest that interventions that support self-esteem, personal mastery, increased social support, and task-oriented coping are promising ways to support transgender youth therapeutically.
Finally, as with all areas of practice that involve diversity, it is important that therapists recognise the limitations of their knowledge and skills and seek supervision and professional consultation from practitioners who are knowledgeable about these issues.
Conclusion
People’s sexual and affiliative behaviour, their interpersonal attractions, and their self-concept and sociocultural identity, are always relevant to their assessment, formulation, and treatment. Working effectively with diverse communities, including working with gender, sexuality and relationship diversity, is a cultural competence, so it is important for therapists to be informed of the issues that are likely to affect the lives of people from the diverse communities with which they work, as well as the distinctive difficulties they might experience. It is hoped that this briefing paper has introduced practitioners to some of the issues faced by people with diverse gender identity and sociosexual attractions, identities and behaviours and therefore increased confidence in working with this aspect of human diversity.
References
Allen D.W. (2013). High school graduation rates among children of same sex-households. Review of Economics of the Household 11: 635–58
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
American Psychiatric Association (2020). What is gender dysphoria? https://www.psychiatry.org/patients-families/gender-dysphoria/what-is-gender-dysphoria
American Psychological Association, Task Force on Appropriate Therapeutic Responses to Sexual Orientation. (2009). Report of the American Psychological Association Task Force on Appropriate Therapeutic Responses to Sexual Orientation. http://www. apa.org/pi/lgbc/publications/therapeutic-resp.html
American Psychological Association. 2005. Lesbian & gay parenting. http://www.apa.org/pi/lgbt/resources/parenting-full.pdf.
American Psychological Association. (2011). Guidelines for psychological practice with lesbian. gay, and bisexual clients. https://www.apa.org/pi/lgbt/resources/guidelines
Annon, J. S. (1976). The PLISSIT model: a proposed conceptual scheme for the behavioral treatment of sexual problems. Journal of sex education and therapy, 2(1), 1-15.
Balsam, K. F., Martell, C. R., Jones, K. P., & Safren, S. A. (2019). Affirmative cognitive behavior therapy with sexual and gender minority people. In G. Y. Iwamasa & P. A. Hays (Eds.), Culturally responsive cognitive behavior therapy: Practice and supervision (p. 287–314). American Psychological Association. https://doi.org/10.1037/0000119-012
Biblarz, T. J., & Stacey, J. (2010). How does the gender of parents matter?. Journal of marriage and family, 72(1), 3-22.
Bilodeau, B. L., & Renn, K. A. (2005). Analysis of LGBT identity development models and implications for practice. New directions for student services, 2005(111), 25-39.
Blumer, Markie L. C. & Y. Gavriel Ansara & Courtney M. Watson (2013) Cisgenderism in Family Therapy: How Everyday Clinical Practices Can Delegitimize People’s Gender Self-Designations. Journal of Family Psychotherapy, 24(4), pp 267-285.
Bradstreet, B., Calver, S., Kent, R., Klein, T., Mitchell, M. B., Parker, D., & Watson, V. (2014). Working therapeutically with LGBTI clients: A practice wisdom resource. National LGBTI Health Alliance: Australia. https://www.beyondblue.org.au/docs/default-source/default-document-library/bw0256-practice-wisdom-guide-online.pdf
British Psychological Society. (2019). Guidelines for psychologist working with gender, sexuality and relationship diversity. https://www.bps.org.uk/news-and-policy/guidelines-psychologists-working-gender-sexuality-and-relationship-diversity
Cass, V. (1979). Homosexuality identity formation: A theoretical model. Journal of Homosexuality, 4, 219–235.
Cass, V. (1984). Homosexual identity formation: Testing a theoretical model. Journal of Homosexuality, 20, 143–167.
Cass, V. C. (1996). Sexual orientation identity formation: A Western phenomenon. In R. Cabaj & T. Stein (Eds.), Textbook of homosexuality and mental health (pp. 227–251). Washington, DC: American Psychiatric Press.
D’Augelli, A. R. (1994). Identity development and sexual orientation: Toward a model of lesbian, gay, and bisexual development. In E. J. Trickett, R. J. Watts, & D. Birman (Eds.), The Jossey-Bass social and behavioral science series. Human diversity: Perspectives on people in context (p. 312–333). Jossey-Bass/Wiley.
Devor, A. H. (2004). Witnessing and mirroring: A fourteen stage model of transsexual identity formation. Journal of Gay & Lesbian Psychotherapy, 8(1-2), 41-67.
Diamond, L. M. (1998). Development of sexual orientation among adolescent and young adult women. Developmental Psychology, 34(5), 1085-1095. https://doi.org/10.1037/0012-1649.34.5.1085
Diamond, L. M. (2006). The evolution of plasticity in female-female desire. Journal of Psychology and Human Sexuality, 18, 245–274. doi:10.1300/J056v18n04_01.
Dillon, F. R., Worthington, R. L., & Moradi, B. (2011). Sexual identity as a universal process. In S. J. Schwartz, K. Luyckx, & V. L. Vignoles (Eds.), Handbook of identity theory and research (p. 649–670). Springer Science + Business Media. https://doi.org/10.1007/978-1-4419-7988-9_27
Edwards, K., & Brooks, A. K. (1999). The development of sexual identity. New directions for adult and continuing education, 1999(84), 49-57.
Erikson, E. (1950). Childhood and society. W. W. Norton.
Fitzgibbons R. P. (2015). Growing up with gay parents: What is the big deal?. The Linacre quarterly, 82(4), 332–336. https://doi.org/10.1179/0024363915Z.000000000120
Flaherty, C. (2019). The trans divide. https://www.insidehighered.com/news/2019/07/19/divide-over-scholarly-debate-over-gender-identity-rages
Grossman, A. H., D’augelli, A. R., & Frank, J. A. (2011). Aspects of psychological resilience among transgender youth. Journal of LGBT youth, 8(2), 103-115.
Gottman Institute. (2021) Same-sex couples. https://www.gottman.com/about/research/same-sex-couples/
Haas, A. P., Eliason, M., Mays, V. M., Mathy, R. M., Cochran, S. D., D’Augelli, A. R., … & Clayton, P. J. (2010). Suicide and suicide risk in lesbian, gay, bisexual, and transgender populations: Review and recommendations. Journal of homosexuality, 58(1), 10-51.
Hamilton, C. J., & Mahalik, J. R. (2009). Minority stress, masculinity, and social norms predicting gay men’s health risk behaviors. Journal of Counseling Psychology, 56(1), 132.
Hammen, C. (2006). Stress generation in depression: Reflections on origins, research, and future directions. Journal of clinical psychology, 62(9), 1065-1082.
Hash, K. M., & Rogers, A. (2013). Clinical practice with older LGBT clients: Overcoming lifelong stigma through strength and resilience. Clinical Social Work Journal, 41(3), 249-257.
ILGA World: Mendos, L. R., Botha, K., Lelis, R. C., López de la Peña, E., Savelev, I., and Tan, D. State-Sponsored Homophobia 2020: Global Legislation Overview Update (December 2020 updated edition). https://ilga.org/downloads/ILGA_World_State_Sponsored_Homophobia_report_global_legislation_overview_update_December_2020.pdf
Kenneady, D. A., & Oswalt, S. B. (2014). Is Cass’s model of homosexual identity formation relevant to today’s society?. American Journal of Sexuality Education, 9(2), 229-246.
Kinsey, A. C., Pomeroy, W. B., & Martin, C. E. (1948). Sexual behavior in the human male. Saunders.
Kinsey Institute (2019). The Kinsey Scale. https://kinseyinstitute.org/research/publications/kinsey-scale.php
Li, G., Kung, K. T., & Hines, M. (2017). Childhood gender-typed behavior and adolescent sexual orientation: A longitudinal population-based study. Developmental Psychology, 53(4), 764.
Lawrence, A. A. (2017). Autogynephilia and the typology of male-to-female transsexualism. European Psychologist, 39-54.
Lehavot, K., & Simoni, J. M. (2011). The impact of minority stress on mental health and substance use among sexual minority women. Journal of consulting and clinical psychology, 79(2), 159.
Lev, A. I. (2004). Transgender emergence: Understanding diverse gender identities and expressions. https://cdn.ymaws.com/www.naswma.org/resource/resmgr/imported/FCE_transgender.pdf
Marks L. (2012). Same-sex parenting and children’s outcomes: A closer examination of the American Psychological Association’s brief on lesbian and gay parenting. Social Science Research 41: 735–51
Martell, C. R., Botzer, M., Williams, M., & Yoshimoto, D. (2003). Gay, lesbian, transgender and bisexual individuals. https://www.dshs.wa.gov/sites/default/files/BHSIA/dbh/documents/gaybestpract.pdf
Martell, C. R., Safren, S. A., & Prince, S. E. (2004). Cognitive-behavioral therapies with lesbian, gay, and bisexual clients. Guilford Press.
Meyer, I. H. (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological bulletin, 129(5), 674.
Meyer, E. J. (2010). Understanding sexuality. In S. R. Steinberg & K. Tobin (Series Eds.), Explorations of educational purpose: Vol. 10. Gender and sexual diversity in schools: An introduction (pp. 47–59). doi:10.1007/978-90-481-8559-7_3
Meyer, I. H., & Frost, D. M. (2013). Minority stress and the health of sexual minorities. In C. J. Patterson & A. R. D’Augelli (Eds.), Handbook of psychology and sexual orientation (p. 252–266). Oxford University Press.
Morgan, E. M. (2013). Contemporary issues in sexual orientation and identity development in emerging adulthood. Emerging Adulthood, 1(1), 52-66.
Pachankis, J. E., & Goldfried, M. R. (2004). Clinical issues in working with lesbian, gay, and bisexual clients. Psychotherapy: Theory, research, practice, training, 41(3), 227.
Palma, T. V., & Stanley, J. L. (2002). Effective counseling with lesbian, gay, and bisexual clients. Journal of College Counseling, 5(1), 74-89.
Pantalone, D. W., Iwamasa, G. Y., & Martell, C. R. (2010). Cognitive-behavioral therapy with diverse populations. In K. S. Dobson (Ed.), Handbook of cognitive-behavioral therapies (p. 445–464). Guilford Press.
Public Health England. (2016). New STI figures show continued increases among gay men. https://www.gov.uk/government/news/new-sti-figures-show-continued-increases-among-gay-men#:~:text=Latest%20figures%20published%20today%20(5,a%2010%25%20increase%20since%202014.
Ritter, K. and Terndrup, A. (2000). Gender role socialization on same-sex couples. Partners Task Force for Gay & Lesbian Couples. https://buddybuddy.com/ritter-1.html
Rochlin, M. (1995). The language of sex: The Heterosexual Questionnaire. In E. D Nelson & B. W. Nelson (Eds.) Gender in the 1990s: Images, realities and issues. Nelson Canada, 38-39.
Rosario, M., & Schrimshaw, E. W. (2014). Theories and etiologies of sexual orientation. In D. L. Tolman, L. M. Diamond, J. A. Bauermeister, W. H. George, J. G. Pfaus, & L. M. Ward (Eds.), APA handbooks in psychology®. APA handbook of sexuality and psychology, Vol. 1. Person-based approaches (p. 555–596). American Psychological Association. https://doi.org/10.1037/14193-018
Savin-Williams, R. C., & Cohen, K. M. (2007). Development of same-sex attracted youth. In I. H. Meyer & M. E. Northridge (Eds.), The health of sexual minorities: Public health perspectives on lesbian, gay, bisexual, and transgender populations (p. 27–47). Springer Science + Business Media. https://doi.org/10.1007/978-0-387-31334-4_2
Serano, J. (2020). Autogynephilia: A scientific review, feminist analysis, and alternative ‘embodiment fantasies’ model. The Sociological Review, 68(4), 763-778.
Smith, M. S., & Gray, S. W. (2009). The courage to challenge: A new measure of hardiness in LGBT adults. Journal of Gay & Lesbian Social Services, 21(1), 73-89.
Storms, M. D. (1980). Theories of sexual orientation. Journal of Personality and Social Psychology, 38(5), 783–792. https://doi.org/10.1037/0022-3514.38.5.783
Su, D., Irwin, J. A., Fisher, C., Ramos, A., Kelley, M., Mendoza, D. A. R., & Coleman, J. D. (2016). Mental health disparities within the LGBT population: A comparison between transgender and nontransgender individuals. Transgender Health, 1(1), 12-20.
Temple Newhook, J., Pyne, J., Winters, K., Feder, S., Holmes, C., Tosh, J., Sinnott, M.-L., Jamieson, A., & Pickett, S. (2018). A critical commentary on follow-up studies and “desistance” theories about transgender and gender-nonconforming children. International Journal of Transgenderism, 19(2), 212–224. https://doi.org/10.1080/15532739.2018.1456390
UK Government (no date). Apply for a Gender Recognition Certificate. https://www.gov.uk/apply-gender-recognition-certificate/print
Wallien, M. S., & Cohen-Kettenis, P. T. (2008). Psychosexual outcome of gender-dysphoric children. Journal of the American Academy of Child & Adolescent Psychiatry, 47(12), 1413-1423.
Worthington, R. L., Savoy, H. B., Dillon, F. R., & Vernaglia, E. R. (2002). Heterosexual identity development: A multidimensional model of individual and social identity. The Counseling Psychologist, 30(4), 496-531.
Appendix 1: Summary of BPS guidelines for psychologists working with gender, sexuality and relationship diversity (2019)
The BPS guidelines state that:
- Psychologists must respect that people from diverse groups have the same rights and responsibilities as the rest of the population
- Psychologists are encouraged to support the self- determination of their clients in the development of their identities, practices and relationships
- Gender, sexuality or relationship diversity are not indicative of a mental disorder
- Psychologists must not engage in ‘reparative’ or ‘conversion’ ‘therapies’
- Psychologists required to make formal assessments should default to respect for a GSRD client’s identity or practice
- Psychologists are encouraged to recognise that attitudes towards gender, sexuality and relationship diversity are located in a changing socio-political context, and to reflect on their own understanding of these concepts
- Psychologists should reflect on the limits
to their practice when working with gender, sexuality and relationship diversity, and consider appropriate referral and training when appropriate - Psychologists should strive to understand the ways in which social stigmatisation (e.g. prejudice, discrimination, and violence) pose risks to gender, sexuality and relationship diverse clients
- Psychologists are encouraged to consider engagement with the wider social and political context regarding gender, sexuality, and relationship diversity in order to reduce social stigma
- Psychologists should be knowledgeable of the diversity of gender, sexuality and relationship identities and practices
- Psychologists general practice should use language which is inclusive of diversity
- Psychologists are encouraged to use the preferred language of gender, sexuality and relationship diverse people
- Psychologists are encouraged to understand the variety of forms of relationships and families of gender, sexuality, and relationship diverse people
- Psychologists should be aware of the potential issues facing gender, sexuality, and relationship diverse clients in their relationships and families
- Psychologists should be mindful of the intersections between gender, sexuality and diverse relationships with other forms of diversity
- Psychologists should recognise and address the particular issues experienced by gender, sexuality and relationship diverse clients with physical and/ or mental health conditions, neurodiversity, and (dis)abilities
- Psychologists should recognise the diversity of developmental pathways for gender, sexuality and relationship diverse people across the lifespan
- Psychologists should recognise the needs and issues of GSRD young people, and their particular vulnerabilities and risks
- Psychologists should recognise and address the needs and issues of GSRD people of working age
- Psychologists are encouraged to recognise the different life experiences of older people in relation to their GSRD identity or practice
- Psychologists should support older GSRD people in their identity or practice, taking due notice of the safety of the client and the context of the clients’ experience
- Psychologists should affirmatively support the partners of older GSRD people
- Psychologists should have sufficient training
in gender, sexuality and relationship diversity that they can work in a respectful and inclusive manner - Psychologists should reflect on their own gender, sexuality and relationships
(c) Andrew Grimmer, 2021
Photo by Steve Johnson from Pexels